
ENDEMIC NIPAH VIRUS KILLED 16 PERSONS IN KERALA INCLUDING NURSE AS IT KILLED MANY IN SILIGURI IN WEST BENGAL
prof .DRRAM,HIV /AIDS,HEPATITIS ,SEX DISEASES & WEAKNESS expert,New Delhi,India, profdrram@gmail.com,+917838059592,+919832025033,ON WHATSAPP
NIPAH VIRUS again isolated at national institute of Virology pune from the samples of initial 3 patient died at Kozikhode at Kerala.Till today it has killed 16 persons and one nursing sister Lini as it likked almost 65 person in my home city Siliguri including staffs of a nursing home and a cardiologist doctor doing echo on an infected person.Although air borne transmission is not seen in this virus but contact by persons or fomites transmit it.
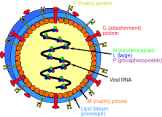
Nipah and Hendra viruses are two related zoonotic pathogens that have emerged in the Asia-Pacific region. Both are RNA viruses that belong to the Paramyxoviridae family. The viruses jump the primary species barrier froma fruit bat and infect a secondary animal host (e.g., pigs or horses), and transmit infections to humans.it infects bth animals and humans and usually cause high mortality.
The natural hosts for the Nipah virus are the fruit bats of the Pteropus genus, which are symptomless carriers. Mainly four species have been demonstrated to have serologic evidence of infection with this virus. The virus is shed in the saliva, urine, semen and excreta of the infected bats.
Nipah virus spreads to humans through direct contact with infected bats, infected pigs, or other people who are infected with the virus. People have been also cautioned to avoid eating fruits that have fallen to the ground.
Nipah virus was first identified in 1998 as the cause of an outbreak of viral encephalitis among pig farmers in Malaysia, where pigs were the intermediate hosts. The virus derives its name from Sungai Nipah, a village in the Malaysian Peninsula where the pig farmers became ill with encephalitis. Since then, several outbreaks of acute Nipah encephalitis have been reported from Bangladesh, West Bengal (Siliguri), India with reports of person-to-person transmission in hospital settings and in the Southern Philippines. Raw date palm sap that had been contaminated by infected fruit bats was identified as the source of infection in an outbreak that occurred in Bangladesh in 2004.
The incubation period is 5 to 14 days.
Clinically, the main presentation of Nipah virus infection is as an encephalitic syndrome characterized by onset of non specific symptoms - sudden onset of fever, headache, myalgia, nausea and vomiting followed by drowsiness, disorientation and mental confusion. The infected person can become comatose within 24 to 48 hours.
The case fatality rate of Nipah encephalitis ranges from 9 to 75%
Meningismus is seen in approximately one-third of patients although marked nuchal rigidity and photophobia are uncommon.Patients infected with Hendra virus have presented with fever and influenza like illnesses, or with meningoencephalitis
Nipah virus infection can be diagnosed by ELISA test.
On MRI, typically multiple, small (less than 5 mm), asymmetric focal lesions in the subcortical and deep white matter without surrounding edema are seen.
There is no effective treatment for Nipah virus infection. The mainstay of treatment is supportive care focusing on managing fever and the neurological symptoms. Infection control practices and barrier nursing are important as person-to-person transmission may occur. Severely ill patients need intensive care.
Ribavirin, a nucleoside analog, can be given empirically as it has a broad spectrum of antiviral activity against both RNA and DNA viruses. In the Malaysian outbreak, 140 treated patients were compared to 54 control patients who did not receive ribavirin. Fewer treated patients died (32% vs 54%). However, treated patients were identified later in the outbreak so it is possible that they were given better general medical care compared to untreated patients seen earlier. Subsequent animal models found that ribavirin, as well as chloroquine, were ineffective.
Anti-thrombotic agents, aspirin and pentoxyfylline, were administered in some patients based upon the recognition that arterial thrombosis may play an important role in the CNS disease.
Nipah virus is classified internationally as a biosecurity level (BSL) 4 agent. So doctors,nursing and parmedical and laboratory and cleaning staff has to take special precautions to prevent its infection and spread while handling these patients..Biosafety Level 4 is required for work with dangerous and exotic agents that pose a high individual risk of aerosol-transmitted laboratory infections and life-threatening disease that is frequently fatal, for which there are no vaccines or treatments, or a related agent with unknown risk of transmission (CDC)
Health ministry has sent a team of ICMR,NII and Animal husbandary to tackle it and State government is also tacking specail measures to isolate those who are in contact and paid rupees twenty lakhs to sister LINI's family who lost her life to protect patients.Ima has also set up a team of expert in that area too and tocheck rumors sothat patints and public donot become panicky.
 Comments (
Comments ( Category (
Category ( Views (
Views (
- Kidney stones universally present hazard in north india,dillution by water prevent it
- Steroid and placebo effect equally for mild persisting asthma with low sputum eosinophils
- Government wants to fix public healthcare staff shortages with ayush docs: will it work?
- Plea in hc for payment of salaries of edmc, north mcd teachers and doctors
- 7 indian pharma companies named in us lawsuit over inflating generic drug prices
- Woman in up dies after explosion in her mouth during treatment,what is diagnosis?
- Woman in up dies after explosion in her mouth during treatment,what is diagnosis?
- Woman in up dies after explosion in her mouth during treatment,what is diagnosis?
- Air pollution ! mothers organising rally in london,anaesthetist choosing gas,will india follow?
- Cardiac arrest is always not sudden as understood -a study
News & Highlights | Articles | Drug Magic | Community Weblog | Health Manager | Testimonials | Video Gallery | Medical Humour
Home | About 'India HeartBeat' | Contact Us | Terms of Use | Privacy Policy | Disclaimer | Advertise With Us | FAQs | Links | Quick Tour